Osteopathy & carpal tunnel syndrome
Anatomy
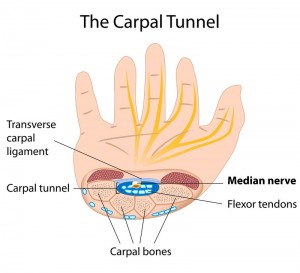
Carpal tunnel syndrome (CTS) is a condition in which the median nerve is compressed as it passes through the wrist, occurring when the carpal tunnel space within the wrist becomes inflamed.
The median nerve is responsible for controlling some of the muscles that move the thumb as well as relaying information back to the brain about the sensations in the thumb, 2nd and 3rd fingers on the palmar surface of the hand.
Women are more likely to develop CTS than men. It affects people of all ages, but it is more common in people over 50 years of age.
Symptoms
Compression of the median nerve causes tingling, pins and needles, numbness and sometimes pain in the affected hand. The symptoms can also be felt in the forearm and/or upper arm. The hand might feel weak, resulting in a patient dropping items or struggling with fine finger movements such as writing, fastening buttons and sewing.
CTS symptoms are typically worse at night and patients often complain of sleep disturbance. Short-term relief can be found by holding the affected hand up in the air, dangling it out of bed or shaking it to reduce the pain and tingling sensation.
The onset of CTS is usually gradual, coming on over a period of weeks.
Causes
The median nerve is sensitive to pressure and below is a list of patient scenarios which increase the risk of developing CTS:
- Fracture of the wrist
- Obesity
- Repetitive (wrist-focused) strain movements (at home and/or in the work place)
- Using vibrating tools (e.g. a pneumatic drill)
- Arthritis (including but not limited to osteoarthritis & rheumatoid arthritis)
- Hormonal changes (e.g. in pregnancy)
- Hypothyroidism / under-active thyroid
Diagnosis
A detailed case history may give clues as to the reason(s) behind a patient’s CTS symptoms.
If the condition is chronic, there may be signs of muscle wasting at the base of the thumb on the affected hand. If the CTS is severe, the thumb, index and middle fingers may be numb to either a light touch (e.g. cotton wool) or a pin prick.
Tinel’s test is carried out by tapping over the pathway of the median nerve on the palmar side of the wrist. Phalen’s test is the alternative, where the patient is asked to bend the palms of the hands towards the forearms (in a prayer-like position) for up to 1-minute. Positive tests reproduce the CTS symptoms in the affected hand(s).
More detailed & reliable nerve conduction testing may help to examine the extent of any median nerve compression. Electrodes are attached to the skin on the fingers and wrist to measure the speed of the median nerve’s response to the current. This testing can show the extent of any nerve damage. The speed at which messages travel between the finger and wrist on the affected hand is slower when the median nerve is damaged.
Ultrasound scans are sometimes employed. The median nerve can become inflamed as it passes through the carpal tunnel, which is visible on a scan. Ultrasound can also show some of the causes of CTS, including swelling in the wrist tendons or joints.
Treatments
There are many different treatments for CTS, all varying in their success rate from patient to patient. For most CTS patients, symptoms worsen over time without some form of treatment and it is therefore important to seek advice in the early stages.
- Osteopathy – osteopathic treatment techniques assist in relieving pressure in the carpal tunnel by stretching soft tissues, alleviating restricted metacarpal and carpal bones, increasing the length of the transverse carpal ligament to enlarge the carpal tunnel, increasing range of motion, strengthening muscles and removing excess fluid – all of which can result in improvements in circulation and median nerve function.
- Bracing / splinting – wearing a brace or splint at night to avoid bending the wrist whilst asleep. Keeping the wrist in a straight and/or neutral position reduces pressure on the median nerve inside the carpal tunnel. In addition, wearing a splint by day whilst carrying out aggravating activities (e.g. computer work / operating a pneumatic drill) may help.
- Non-steroidal anti-inflammatory drugs (NSAIDs) – medications such as (over the counter) ibuprofen and (prescription) naproxen can help to relieve pain and inflammation at the wrist.
- Modification of activity – CTS symptoms often occur when the hand and wrist are flexed or extended for prolonged periods. Taking regular breaks or modifying aggravating work and/or recreational activities can help to slow down the progression of CTS.
- Nerve gliding exercises – the aim of these exercises is to allow the median nerve to move more freely (‘breathe’) within the confines of the carpal tunnel.
- Steroid injections – corticosteroid is a powerful anti-inflammatory agent that can be injected into the carpal tunnel to relieve CTS symptoms, however the effect is sometimes only temporary.
- Open carpal tunnel release – a small incision is made into the palm of the hand and the transverse carpal ligament (the roof of the carpal tunnel) is divided. This increases the size of the tunnel and decreases pressure on the median nerve. After surgery, the ligament may gradually grow back together, but there will be more space within the carpal tunnel and pressure on the median nerve is relieved.
- Endoscopic carpal tunnel release – here one or two smaller skin incisions (portals) are made and a miniature camera (an endoscope) is inserted to see inside the hand and wrist. The transverse carpal ligament is again divided.